SMS marketing for pharmacies means sending text messages to patients who have consented to receive them – from prescription pickup alerts to refill reminders, appointment confirmations, to health campaigns. Done well, it shortens the path between patient and pharmacy, improves medication adherence, and reduces no-shows. Done poorly, it triggers HIPAA violations, TCPA class actions, or GDPR penalties running anywhere from $500 per message to seven-figure corporate fines.
The stakes have risen in the last eighteen months. The FCC’s 1-to-1 consent rule took effect in January 2025. Mandatory 10DLC registration followed in February 2025. HIPAA’s Security Rule update the same month removed the addressable exception for encryption. TCPA class action filings rose 112% YoY in Q1 2025 alone. The compliance bar is higher than it was two years ago, and pharmacies that treated texting as a casual tool are the most exposed.
This guide is primarily for US pharmacies – independent operators, regional chains, and marketing leads at larger groups – with a secondary lens on EU operations, where GDPR and ePrivacy add their own requirements. You’ll learn what messages you can send without marketing consent, what requires an explicit opt-in, what belongs in the message body and what doesn’t, and how to run campaigns that actually improve patient outcomes instead of just filling an inbox.
The case for SMS in pharmacy: Beyond marketing, into patient outcomes
The most persuasive argument for pharmacy SMS isn’t engagement metrics but actual clinical evidence. A meta-analysis of 16 randomized controlled trials (N=2,742) found that text messaging doubled the odds of medication adherence (OR 2.11, P<0.001) and increased overall adherence rates by 17.8 percentage points. We’re looking at a treatment-efficacy intervention delivered by SMS!
The scale of the problem is what makes this finding significant. Only about 50% of patients with chronic illness take their medications as prescribed, according to WHO estimates cited in recent JMIR research.
Non-adherence drives hospital readmissions, worsened outcomes, and – from the pharmacy’s perspective – missed refills. When an SMS reminder moves adherence by 17.8 points, it moves refill revenue at the same time. The business case and the clinical case go hand in hand.
Two nuances from the research are worth internalizing before you build campaigns. Tailored messages outperform generic ones. A reminder that references the patient’s regimen context does more than “time to take your pill”. Longer campaigns (6+ months) outperform short bursts, according to 2025 work in Frontiers in Pharmacology. Adherence isn’t a one-shot intervention. It’s a relationship maintained by small, consistent touches.
SMS is also the channel that doesn’t require anything from the patient beyond a working phone. 98% of SMS notifications are read, 90% within three minutes of delivery. 97% of US smartphone owners use text messaging, and the figure barely drops among patients over 50 which is the demographic most likely to be managing chronic conditions and visiting a pharmacy regularly.
💡 For a pharmacy patient base, SMS reaches closer to 100% of the addressable population than any other digital channel.
Transactional vs. marketing SMS: The distinction that determines your consent requirements
Before building any campaign, get one classification right: is this message transactional or marketing? The answer determines which consent rules apply, what language you need, and what the regulator will ask you to prove if something goes south. The line looks obvious in theory but gets blurry fast in practice.
A transactional SMS supports an existing healthcare relationship and the care the patient is already receiving. Prescription ready alerts, refill reminders, appointment confirmations, delay notifications.
Under TCPA, these require prior express consent – a lower bar than marketing, typically satisfied when the patient provides their number in the context of care. HIPAA treats them as healthcare communications, which means they can be sent without explicit marketing authorization, provided the message itself doesn’t expose Protected Health Information.
A marketing SMS promotes a product, service, or offering. Seasonal campaigns, new service announcements, wellness promotions, discount notifications.
Under TCPA, these require prior express written consent – specifically, a signed disclosure that names your pharmacy, discloses the marketing purpose, and is not bundled with other agreements. This is a materially higher bar, and the FCC’s 1-to-1 consent rule (effective January 2025) tightened it further: consent collected through lead-generation sites that list multiple brands is no longer valid. Each business must independently collect consent under its own name.

The table below maps the typical pharmacy use cases:
| Use case | SMS type | Marketing consent required? |
|---|---|---|
| Prescription ready for pickup | Transactional | ❌ No |
| Refill reminder (approaching end of supply) | Transactional | ❌ No |
| Appointment reminder (vaccination, consultation) | Transactional | ❌ No |
| Out-of-stock / delay notification | Transactional | ❌ No |
| Seasonal health campaign (flu shots available) | Marketing | ✅ Yes |
| New pharmacy service announcement | Marketing | ✅ Yes |
| Discount, promotion, or loyalty offer | Marketing | ✅ Yes |
| Health education tied to a service you sell | Marketing | ✅ Yes |
❗Two practical rules carry most of the weight.
First, the moment a message encourages the patient to purchase or use a product or service, it becomes marketing. That’s the test. “Your prescription is ready” is transactional. “Your prescription is ready – make sure to ask about our new immunization service” is marketing. The second half of that sentence converted the entire SMS.
Second, don’t mix transactional and marketing content in the same message. Regulators and courts generally classify mixed messages as marketing in their entirety, which means a careless add-on to a pickup alert creates a TCPA violation for every patient who hasn’t signed a marketing consent. The conservative approach is a clean split: one channel for care communications, another for promotional sequences, and a firewall between them in your content calendar.
One more distinction matters for US pharmacies that doesn’t exist cleanly in the EU framework: the HIPAA marketing definition. Under HIPAA, a “marketing” communication about a third-party product or service generally requires a separate written authorization even if you already have TCPA consent.
Communications about your own services (a new medication therapy management program, a vaccination clinic at your location) fall under treatment or healthcare operations and don’t need that additional HIPAA authorization. This is where pharmacy legal counsel earns its fee: mapping each campaign against both the TCPA consent framework and the HIPAA authorization framework before anything ships.
US compliance framework: HIPAA, TCPA, and the carrier layer
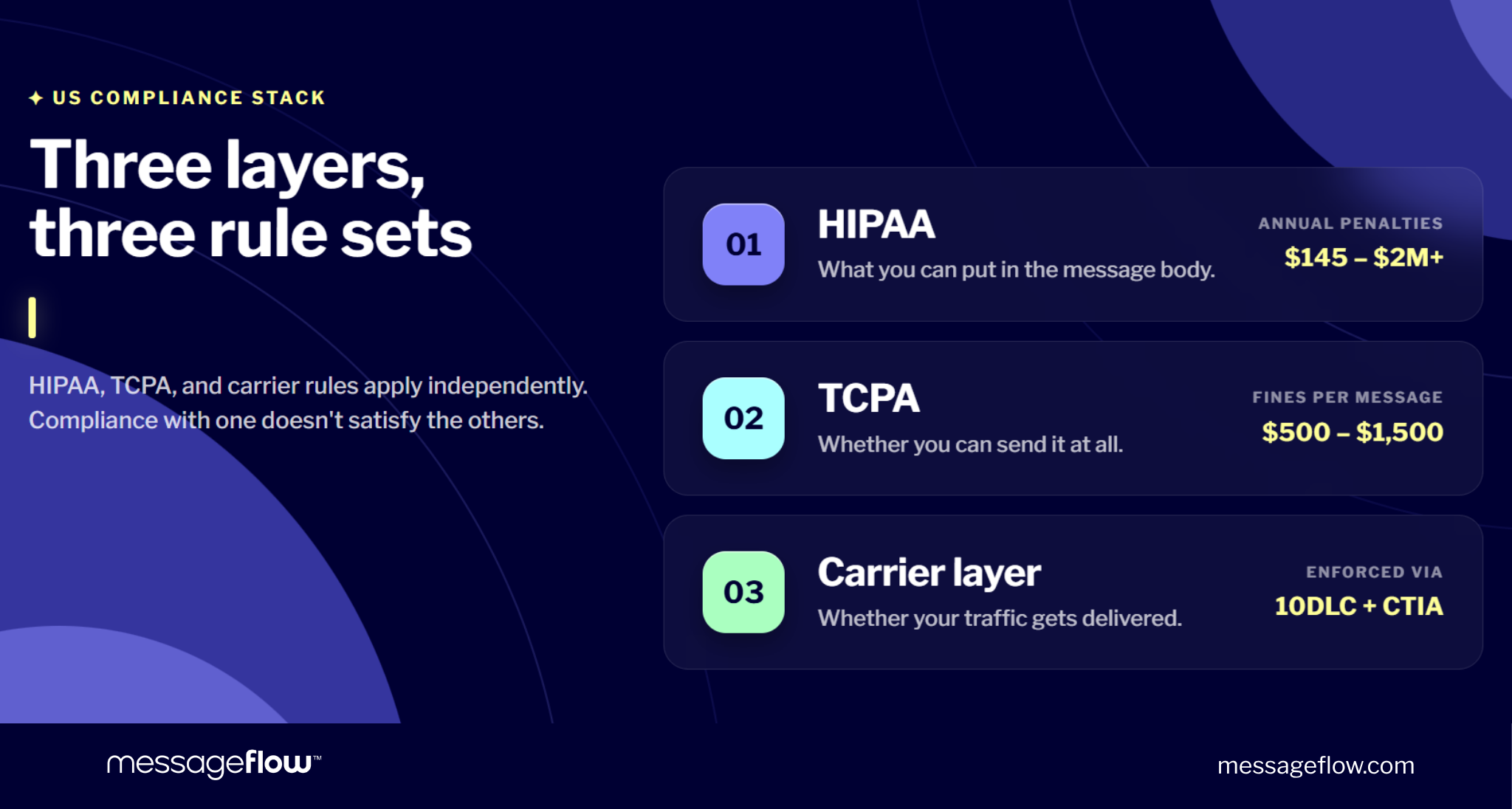
US pharmacy SMS compliance is complex because three distinct regulatory systems stack on top of each other. HIPAA governs what you can say in the message. TCPA governs whether you can send it at all. The carrier layer (10DLC registration and CTIA guidelines) governs whether your traffic will be delivered. Each has independent penalties, and compliance with one does not satisfy the others.
HIPAA: What you can put in the message body
Pharmacies are HIPAA-covered entities. Every SMS that contains Protected Health Information (PHI) such as medication names, dosages, diagnoses, insurance details, treatment information, must be handled under HIPAA safeguards. Standard SMS does not meet those safeguards. It travels unencrypted across carrier networks, lacks audit trails, and offers no access controls on the recipient device.
The practical consequence is a rule that trips up pharmacies constantly: no PHI in the body of a standard SMS. A message reading “Your prescription is ready for pickup” is compliant. A message reading “Your Metformin 500mg refill is ready” exposes a diagnosis by implication and violates HIPAA. The distinction sounds minor but the regulators do not see it as such.
Two changes from January 2025 sharpened the picture. The HIPAA Security Rule update removed the “addressable” designation for encryption requirements, making AES-256 encryption at rest and TLS 1.3 in transit mandatory rather than conditional for all electronic PHI. And the HHS enforcement data continues to show annual HIPAA penalties ranging from $145 to over $2 million per entity depending on severity and willfulness.
If your use case genuinely requires PHI in the message – specialty pharmacy communications, some medication therapy management programs – you need two things: a Business Associate Agreement (BAA) with your messaging platform, and a platform architected for HIPAA. Not every SMS vendor qualifies. Verify the BAA is specific to messaging, not a generic technology BAA, and that the platform’s encryption, audit logging, and access controls are documented.
💡 For the common pharmacy use cases involving pickup alerts, refill reminders, appointment confirmations the cleaner approach is to strip PHI from the message entirely. “Your medication is ready” works. The patient already knows what they picked up.
TCPA: The consent framework that drives class actions
The Telephone Consumer Protection Act governs whether you can send the message. Penalties run $500-$1,500 per non-compliant message, and because TCPA supports class actions, a single misfire to 10,000 patients can become a nine-figure exposure. 507 TCPA class actions were filed in Q1 2025 alone – a 112% increase YoY, driven largely by the FCC’s tightened consent rules.
TCPA draws the same transactional-versus-marketing line discussed earlier, with different consent standards for each:
Transactional / healthcare messages require prior express consent. In practice, this is satisfied when the patient provides their phone number in the context of the care relationship by filling out a new patient form, requesting a prescription transfer, scheduling a vaccination. The consent doesn’t need to be written, but it does need to be documented.
Marketing messages require prior express written consent. This, in TCPA terms, includes electronic signatures, checkbox consents on a digital form, and keyword opt-ins (“text HEALTH to 12345”). What it cannot be: bundled into terms of service, pre-checked, implied from an existing customer relationship, or obtained through a third party that lists multiple brands.
That last point is the 1-to-1 consent rule, effective January 2025. Lead generation sites that collected consent for “our partners” or “affiliated businesses” stopped producing valid TCPA consent on that date.
💡 Each business must collect consent independently, under its own name, for its own communications. If your pharmacy inherited a marketing list from a broader healthcare network or acquired it through a third party, that list likely does not meet the current standard.
Opt-out handling is a separate compliance surface. TCPA requires processing opt-outs within 10 business days. Best practice and CTIA guidance both push immediate. The standard keyword is STOP, but platforms should also honor UNSUBSCRIBE, QUIT, END, and CANCEL. Re-subbing a patient who texted STOP, even accidentally, through a list sync error, is itself a TCPA violation.
One healthcare-specific nuance: HIPAA-covered entities sending care-related messages qualify for a narrower consent standard under the TCPA healthcare exemption. This does not override the marketing / transactional line – promotional messages still require prior express written consent – but it clarifies that prescription alerts and appointment reminders fall under the lower consent bar.
The carrier layer: 10DLC and CTIA
Even with perfect HIPAA and TCPA compliance, US carriers can still throttle or block your traffic if the carrier layer isn’t addressed. Since February 3, 2025, all Application-to-Person (A2P) SMS traffic in the US must be registered under 10-Digit Long Code (10DLC). Registration happens through The Campaign Registry and requires:
- Brand registration (your pharmacy’s legal identity, EIN, contact information)
- Campaign registration (the use case – appointment reminders, marketing, mixed)
- Sample message content demonstrating compliance
Unregistered traffic is throttled, blocked, or silently dropped by carriers. Pharmacies don’t usually register directly – the SMS platform handles it – but you should verify registration is active and that your campaign use cases are correctly classified. Misclassifying a marketing campaign as transactional on your 10DLC registration is its own compliance problem.
CTIA guidelines sit alongside 10DLC as a carrier-enforced code of conduct. The requirements that trip pharmacies up most often:
- Brand identification in every message. “[Pharmacy Name]:” at the start of the SMS.
- Throughput limits tied to your 10DLC tier. Each campaign is assigned a daily message ceiling based on brand trust score and vetting tier. Large seasonal sends can hit it and drop.
- No public URL shorteners. Bit.ly, tinyurl, and similar are flagged as suspicious. Carriers increasingly block them. Use branded short links or domain-rooted links.
- No SHAFT content. Sex, Hate, Alcohol, Firearms, Tobacco – all restricted. Pharmacies rarely trip this but smoking cessation campaigns can sit adjacent to the tobacco restriction and need careful language.
EU perspective: GDPR and the two-layer consent model
For pharmacies operating in the EU or US pharmacies serving EU patients the framework shifts significantly. GDPR governs the processing of personal data (including phone numbers), and the ePrivacy Directive governs electronic marketing communications. These are two independent consent layers and both must be satisfied before a marketing SMS goes out.
GDPR’s Article 6 provides the lawful basis for processing the phone number itself. For an existing patient, processing can often be grounded in legitimate interests (Article 6(1)(f)) for care-related communications. For marketing, you generally need explicit consent (Article 6(1)(a)). Pre-ticked boxes are invalid, bundled consents are invalid, and consent must be as easy to withdraw as it was to give.
The ePrivacy layer adds a channel-specific consent requirement. Opting into email marketing does not authorize SMS marketing. In practice, EU-compliant opt-in forms list each channel separately, with independent checkboxes, none pre-checked.
The health data issue is stricter in the EU than in the US. GDPR Article 9 classifies data concerning health as a “special category” requiring explicit authorization for processing. Sending an SMS that reveals a patient takes a specific medication, even through implication, processes health data in a channel that generally doesn’t meet Article 9’s safeguards. The rule is the same as HIPAA in practice: keep medication names and health details out of standard SMS bodies.
UK pharmacies operate under UK GDPR and PECR (Privacy and Electronic Communications Regulations), with one meaningful difference: PECR’s “soft opt-in” allows marketing to existing customers for similar products and services without fresh consent, provided the customer had a clear opt-out opportunity at collection.
The UK Data Use and Access Act (August 2025) confirmed this framework. For pharmacies with UK and EU operations, the practical rule is to build to the stricter EU standard and let the UK operation benefit from the same infrastructure.
A practical disclaimer applies across all jurisdictions covered here: this is general guidance, not legal advice. Consent language, retention policies, and authorization requirements need to be reviewed by counsel familiar with your specific operation, especially for pharmacies operating across state or national borders, where overlapping rules can produce unexpected combinations.
How to build a compliant opt-in system
The consent infrastructure is where many pharmacy SMS programs either quietly succeed or quietly fail. The rules discussed so far only matter if your collection process, documentation, and opt-out handling actually hold up under audit. Three decisions shape whether they do.
Separate the two consent triggers at the source
The first decision is architectural: treat care communications and marketing communications as two distinct opt-ins from day one, collected at different moments, documented separately, and managed in independent suppression lists.
Care communication opt-in is captured at the point the patient enters the care relationship – new patient intake, prescription transfer request, first appointment booking. The consent is narrow, tied to the specific care interaction, and often satisfies TCPA’s prior express consent standard simply by virtue of the patient providing their number in that context. Document it anyway: date, form used, patient signature or checkbox record.
Marketing opt-in is captured separately, always with an affirmative action from the patient, never bundled with anything else. The consent language must name your pharmacy specifically (post-January 2025 FCC rule), disclose that messages will be promotional in nature, state message frequency expectations, and provide an easy opt-out mechanism.
Pharmacies that collapse these into a single “I agree to receive communications” checkbox end up with two problems. Their care communications are probably fine, but their marketing consent is likely invalid because TCPA requires the marketing purpose to be clearly disclosed and separately agreed to. And when a patient complains or a regulator asks, there’s no way to prove which consent the patient gave.
Design compliant collection touchpoints
Five touchpoints cover most of the collection opportunities for a typical US pharmacy:
Point-of-sale tablet or terminal. A digital form at the counter is the cleanest option. It captures timestamp, IP, consent language version, and the patient’s affirmative action on a single record. Separate checkboxes for transactional and marketing consent, neither pre-checked.
Pharmacy website or patient portal. Standard web form with independent checkboxes. The FCC’s 1-to-1 rule means the consent must be for your pharmacy specifically, not for “our network” or “our partners.” If you operate multiple brands, each brand needs its own consent.
Keyword opt-in via SMS. “Text WELLNESS to 12345 to receive health tips from [Pharmacy Name].” This is a clean mechanism because the patient’s inbound message itself is the consent record. Pair with a confirmation message that restates the subscription terms and the opt-out instruction.
Appointment or vaccination booking. Natural touchpoint with high relevance. The patient is already in a care interaction. Separate the marketing consent from the booking confirmation. Don’t condition service on marketing agreement.
Ecommerce checkout. Optional checkbox at order confirmation, never required to complete the purchase. The disclosure language must meet the full TCPA standard.
Here’s a ready-to-adapt template for US marketing consent:
By providing your mobile number and checking the box below you agree to receive recurring marketing text messages from [Pharmacy Name] at the number provided. Messages may include health promotions, new service announcements, and seasonal wellness campaigns. Consent is not a condition of purchase. Message frequency varies, message and data rates may apply. You may request to be unsubscribed at any time. See our Privacy Policy at [URL] and Terms at [URL].
[ ] I agree (unchecked by default)
The template above reflects current TCPA and CTIA expectations. EU and UK versions need GDPR-specific wording, particularly around data controller identification, retention periods, and withdrawal rights, and should be drafted with counsel familiar with ePrivacy requirements.
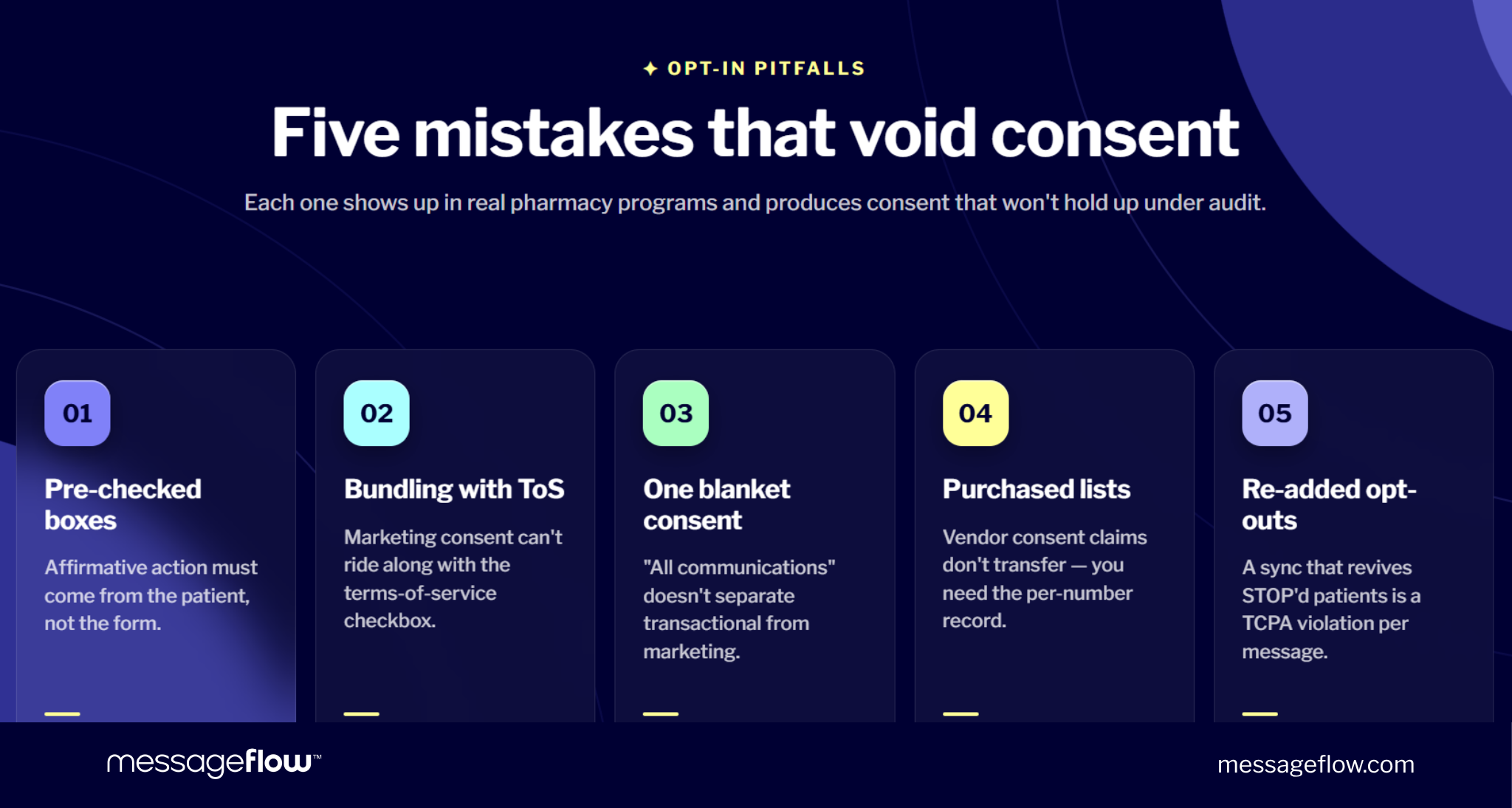
Five opt-in mistakes that invalidate consent
All five appear in real pharmacy programs regularly and produce consent that won’t hold up:
Pre-checked boxes. Invalid under TCPA, GDPR, and CASL. The patient must take an affirmative action, and that action must be theirs, not yours.
Bundling marketing consent with terms of service. A patient agreeing to your terms of service is not agreeing to marketing SMS, regardless of what the terms say. Marketing consent must be separately presented and separately agreed to.
Single consent covering all message types. A checkbox reading “I agree to receive communications from [Pharmacy]” does not distinguish transactional from marketing, and regulators will generally resolve that ambiguity against you. Separate the consents.
Purchasing lists without documented individual consent. A vendor’s assurance that their list is opt-in does not transfer. TCPA and GDPR both require you to hold the consent record for each individual number you message. Inherited or purchased lists rarely meet this standard.
Re-subscribing patients who opted out. Once a patient texts STOP, they cannot receive marketing from you again until they affirmatively opt back in. A list sync that accidentally re-adds opted-out numbers is a TCPA violation for every message sent, and courts do not accept “our CRM did it” as a defense.
Double opt-in: When the extra friction pays for itself
Double opt-in adds a confirmation step. After the patient ticks the initial checkbox, they receive an SMS asking them to confirm (“Reply YES to confirm your subscription to [Pharmacy] health updates”). Only confirmed numbers enter the active list.
The trade-off is real. Single opt-in produces larger lists. Double opt-in produces smaller, higher-quality lists with stronger consent records. For most US pharmacy use cases where TCPA penalties run $500-$1,500 per message and class actions can multiply that exposure by tens of thousands, the stronger consent record is worth the lower conversion.
Double opt-in is particularly valuable in three situations: online consent collection (where typos and incorrect numbers are common), acquisition from a new marketing channel where you don’t yet trust the consent quality, and high-frequency campaigns where a compliance challenge would be most damaging.
For in-person consent at the pharmacy counter, where the patient provides the number face-to-face, single opt-in usually provides adequate protection.
For EU pharmacies, double opt-in is closer to a default. GDPR’s consent evidentiary standard is high enough that the second confirmation step substantially strengthens the defensibility of the consent record. Most reputable EU-operating platforms recommend it as standard practice.
What to send: SMS marketing for pharmacies templates that work
Below are templates for the core pharmacy use cases, grouped by consent category. They’re written to meet current US compliance standards – brand identification at the start, opt-out at the end, no PHI in the body – and adapt cleanly to EU requirements with minor language adjustments.
Transactional messages (no marketing consent required)
These support the care relationship and don’t require written marketing consent. They still require prior express consent (typically satisfied when the patient provides their number in a care context) and still must avoid PHI in the message body.
Prescription ready for pickup
Refill reminder
Appointment reminder (vaccination)
Prescription delay notification
Two things worth noticing across all four. First, none of them name the medication, the condition, or any detail that would identify what the patient is being treated for. “Your medication” carries the entire informational load and that’s enough, because the patient already knows what they filled. Second, each template identifies the pharmacy at the start and includes an opt-out, even though opt-out isn’t strictly required for transactional messages. The redundancy costs nothing and signals compliance-first design to carriers, who weigh this in deliverability scoring.
Marketing messages (written consent required)
These promote a service, announce a new offering, or encourage use of a product. All require TCPA-compliant prior express written consent and, for US pharmacies, should go only to patients who signed the marketing-specific opt-in discussed earlier.
Seasonal health campaign
New service announcement
Health education tied to a service
Adherence support (marketing-consented)
The adherence template sits on a line worth understanding. A refill reminder to an active prescription is transactional. A re-engagement message to a patient who has lapsed is closer to marketing – you’re encouraging a return to a service relationship that has paused. The conservative classification is marketing, which means this message only goes to patients who opted in to promotional communications. That’s the classification most compliance counsel will advise.
Adherence sequences: The highest-value use case
The clinical evidence around SMS and medication adherence points at a specific design pattern: a series of touches anchored to the patient’s refill cycle, not one-off blasts. A sequence that tends to work:
Day 0 (prescription dispensed, transactional): Confirmation and pickup acknowledgment. No marketing consent needed.
Day 25 (approaching refill, transactional): “Your refill is due in the next few days. Request online or call us.” Still transactional because it supports the existing prescription.
Day 32 (refill lapsed, still transactional): “We haven’t heard from you about your refill. Reply REFILL or call 555-0100 if you’d like to continue.” Care-related, no marketing pitch.
Day 60 (patient has lapsed, marketing consent required): “Haven’t seen you in a while. Our pharmacist is available for a free consultation about managing your medications. Call 555-0100.” This one needs marketing consent because it’s re-engagement, not refill logistics.
💡 The split between Day 32 and Day 60 is where pharmacies often get the classification wrong. A message framed as a check-in after a specific lapsed prescription is defensibly transactional. A message framed as a general “come back to us” invitation is marketing. Design the sequence with that distinction in mind and route each step to the consent list that matches.
What not to send: Categories that create exposure
Some types of SMS messages are either outright non-compliant or sit close enough to the line that the risk-adjusted return is negative:
- Messages containing medication names, diagnoses, or dosages – HIPAA exposure regardless of consent status.
- Third-party product promotions (e.g., a manufacturer’s campaign routed through your list) – triggers HIPAA’s marketing authorization requirement on top of TCPA.
- Urgent-sounding messages designed to pressure action – “Don’t miss out” framing in healthcare contexts attracts both regulatory and reputational scrutiny.
- Messages to patients who opted out – every message after opt-out is a separate TCPA violation, including messages that resulted from a failed sync between systems.
- SHAFT content (Sex, Hate, Alcohol, Firearms, Tobacco) – blocked at the carrier layer. Smoking cessation campaigns need careful language to avoid tobacco-adjacent flagging.
- Public URL shorteners (bit.ly, tinyurl) – increasingly blocked as suspicious. Use branded or domain-rooted links instead.
Implementation checklist: From platform selection to first campaign
Six steps move a pharmacy from “we should probably text patients” to a live, compliant program. The order matters too. Reversing step 1 and step 3, for example, usually means redoing step 1.
Step 1: Select a platform that meets pharmacy-specific requirements
Platform selection determines most of the downstream compliance posture so this decision deserves more scrutiny than it typically gets. For pharmacies, the following requirements are non-negotiable:
A signed Business Associate Agreement (BAA) specific to messaging, not a generic technology BAA. Required if you’ll ever send PHI, advisable even if you won’t, because the BAA signals that the platform has been built for healthcare-grade security.
Automated 10DLC registration handled by the platform (applicable in the US). You shouldn’t be managing Campaign Registry submissions manually. The platform should register your brand and campaign use cases and maintain the registration over time.
Consent logging with audit trail – timestamp, consent wording version, collection channel, patient identifier. In a regulatory challenge, the audit log is the evidence.
Direct carrier connections where available. For US traffic, this means established relationships with the Tier 1 carriers. For EU traffic, direct interconnect with local mobile network operators matters for deliverability and cost.
Step 2: Register 10DLC (US) or Sender ID (EU / global)
For US operations: register your brand and campaign use cases through The Campaign Registry. Required since February 3, 2025. The platform typically handles submission, but verify two things: the campaign use case is correctly classified (marketing vs. account notification vs. mixed) and the brand registration reflects your legal pharmacy entity, not a parent company or franchise group.
Misclassified registrations are a quiet compliance problem. A marketing campaign registered as “account notification” to get past carrier filters is a provable violation if discovered, and carriers increasingly audit registration accuracy.
For EU and global operations: register an alphanumeric Sender ID – up to 11 characters – with the relevant carriers. The Sender ID replaces a phone number as the message source, improving brand recognition and reducing the chance patients dismiss the SMS as spam. Good examples: RxCenter, HealthRx, PharmFirst. Avoid numeric-only or cryptic strings, recognition matters more than cleverness.
Step 3: Build your consent database
Before any campaign ships, audit what you already have. For each contact in your patient database answer two questions: do I have a documented consent record for this number and does that consent authorize the category of message I want to send?
💡 For US marketing consent, the audit is particularly strict. Consents collected before January 2025 may not meet the FCC’s 1-to-1 rule if they were obtained through a network, lead-gen site, or parent-brand framing. Consents bundled with terms of service are invalid. Consents for “communications” without a clear marketing disclosure are invalid for marketing purposes.
Build the consent log with these fields as a minimum: patient identifier, phone number, consent type (transactional / marketing), date collected, collection channel, consent wording version, and IP or device metadata where applicable. When a patient opts out, log the date and keep the record. Evidence that the opt-out was processed is as important as evidence of the original consent.
Sync opt-outs in real time across every system that touches the patient. A CRM, a point-of-sale system, an ecommerce platform, and an SMS platform that don’t share a suppression list will eventually re-subscribe someone who texted STOP, and that’s a TCPA violation on every message that follows.
Step 4: Write message content that passes three filters
Every SMS should clear three checks before it goes out:
Compliance filter. No PHI in the body. Brand identification at the start. Opt-out instruction at the end (always for marketing; recommended for transactional). No SHAFT-adjacent language. No public URL shorteners.
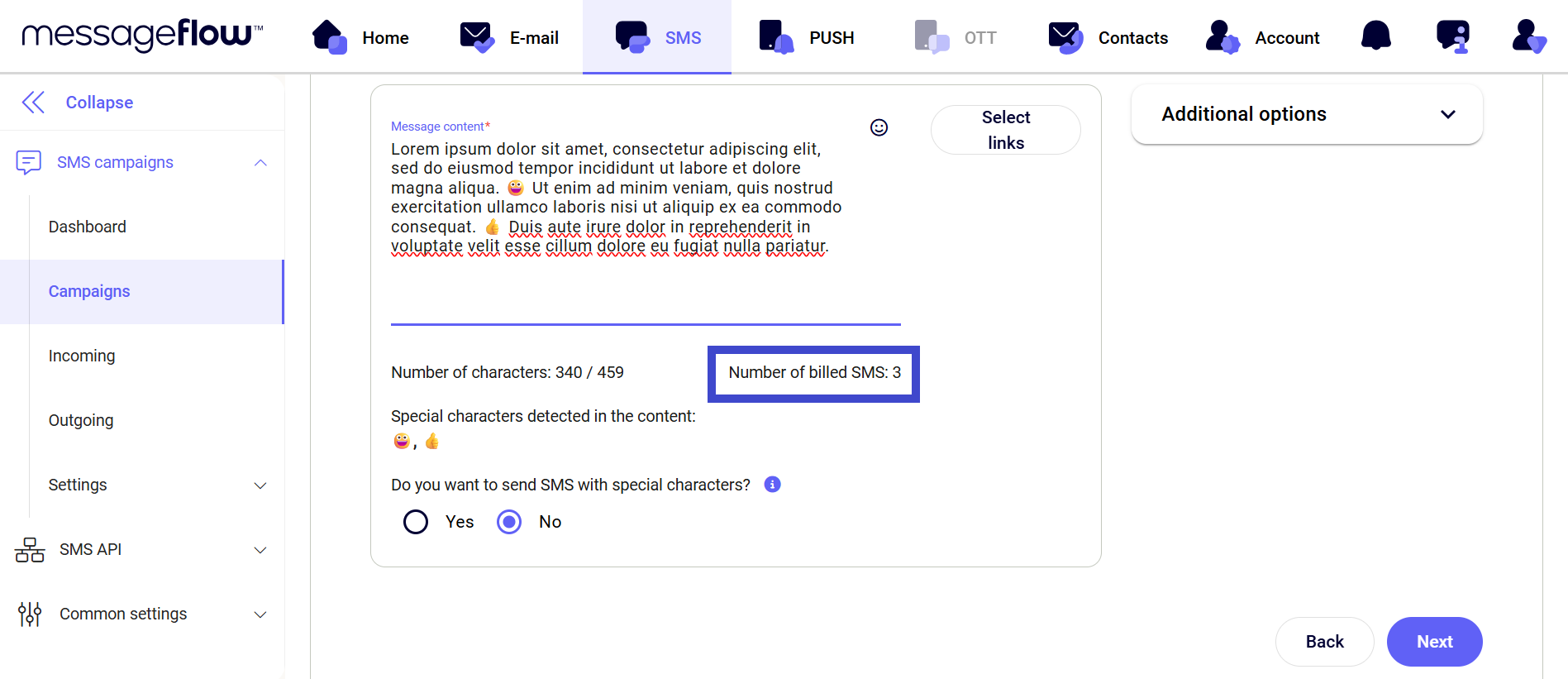
Character budget filter. 160 characters in GSM-7 encoding = one SMS = one billing unit. Anything longer splits into multiple messages at multiple costs. Special characters (emoji, curly quotes, em dashes) can push a message into Unicode encoding, which drops the per-message limit to 70 characters. Most platforms flag this in their composer, don’t ignore the warning.
Clarity filter. One message, one purpose. A pickup alert is a pickup alert. An appointment reminder is an appointment reminder. Combining purposes saves no money and creates classification ambiguity.
Step 5: Set timing and frequency rules
US-specific optimal timing for SMS: TCPA prohibits marketing messages between 9pm and 8am in the recipient’s local time zone. Several states are stricter. Alabama and Louisiana prohibit calls and texts outside 8am-8pm, and some state laws extend the quiet hours further on weekends. Configure the platform to respect recipient time zones, not the sender’s, and build in state-specific overrides where required.
General best practice: marketing engagement peaks Tuesday through Thursday, 10am-5pm local time. Monday is consumed by accumulated weekend tasks, Friday afternoon through Sunday reads as intrusion in healthcare contexts. Transactional messages (pickup alerts, appointment confirmations) can run whenever the underlying event requires, though even these should avoid overnight hours unless operationally essential.
Frequency: 2-4 marketing messages per month per patient is a reasonable upper bound. Beyond that opt-out rates climb and engagement falls. Transactional messages don’t count against this limit but shouldn’t stack unnecessarily. If a patient gets a pickup alert, a next-day reminder, and a third-day reminder, the third message is closer to nagging than service.
Step 6: Measure what actually matters
Five metrics cover the full picture for a pharmacy program:
Delivery rate. Healthy programs run above 98%. Drops below that signal platform issues, carrier filtering problems, or deteriorating list quality (disconnected numbers, invalid formats).
Open and read rate. SMS baseline is 90%+ within a few minutes of delivery. This isn’t usually the metric that varies campaign-to-campaign.
Click-through rate on links. Tag every link with UTM parameters so downstream attribution in web analytics works. For healthcare SMS, 10-25% CTR is a reasonable range. Benchmarks vary significantly by campaign type and patient segment.
Refill or appointment conversion. The metric that matters commercially. Track refills requested or appointments booked within 7-14 days of the campaign, against a pre-campaign baseline. Without this, you’re optimizing engagement metrics that may not translate to pharmacy outcomes.
Opt-out rate. Below 1% per campaign is healthy. Above 1% is a warning sign typically indicating frequency issues, segment mismatch, or message-content problems. Above 2% warrants pausing the program and investigating before shipping the next campaign.
MessageFlow supports pharmacies with carrier-direct connections, multichannel campaigns across SMS, email, RCS, and push, and a single dashboard for compliant outreach. Learn more about the platform or talk to the team about your specific use case.
In summary
Pharmacy SMS has evolved past the “should we do it” question. With adherence meta-analyses showing doubled odds of patient compliance and penalty exposure running $500-$1,500 per non-compliant message in the US, the decision is no longer whether to text patients but whether to build a program that delivers clinical outcomes under a compliance framework that will hold up, or to keep sending messages from an informal setup that exposes the pharmacy to meaningful risk.
Pharmacies that get the consent architecture right, keep PHI out of message bodies, register 10DLC correctly, and design campaigns around adherence rather than volume will see the benefits compound.
Refill rates improve, no-shows drop, and the patient relationship shifts from transactional visits to an ongoing care conversation. Those that treat SMS as a quick marketing channel without the compliance infrastructure will find the exposure catches up, usually at the worst possible moment.
Ready to launch patient-first, compliant SMS campaigns for your pharmacy? Talk to the MessageFlow team – we work with pharmacy operators to build programs that meet current regulatory standards without slowing down the rollout.
This article provides general guidance on pharmacy SMS marketing and is not legal advice. Regulatory requirements differ by jurisdiction and by specific business context. Consult qualified legal counsel familiar with your pharmacy’s operations – particularly around TCPA, HIPAA, GDPR, and state-level rules – before finalizing consent language or launching campaigns. Information reflects the regulatory landscape as of May 2026.
FAQ: Answering questions on SMS marketing for pharmacies
Yes, with appropriate consent. In the US, marketing SMS requires TCPA-compliant prior express written consent – a separate, clearly-disclosed opt-in that names your pharmacy specifically. Transactional messages (prescription alerts, appointment reminders) require only prior express consent, typically satisfied when the patient provides their number in a care context.
EU pharmacies need explicit GDPR consent plus separate ePrivacy consent for the SMS channel. Rules vary meaningfully by jurisdiction, so multi-region operators should build to the strictest applicable standard.
Not in standard SMS. Medication names constitute Protected Health Information under HIPAA in the US, and health data under GDPR Article 9 in the EU – both categories requiring stronger safeguards than unencrypted SMS provides. “Your Metformin 500mg refill is ready” violates both frameworks. “Your medication is ready for pickup” is compliant and carries the same practical information for the patient.
HIPAA-compliant encrypted messaging platforms allow PHI in specific use cases but require a signed Business Associate Agreement and platform-level safeguards that standard SMS lacks.
A transactional SMS supports an existing care relationship like prescription alerts, refill reminders, or appointment confirmations. It requires prior express consent under TCPA, typically satisfied at patient intake.
A marketing SMS promotes a product or service like seasonal campaigns, new service announcements, or promotional offers. It requires prior express written consent under TCPA, which means a separate, clearly-disclosed opt-in.
The classification is determined by whether the message encourages use of a product or service. Mixing transactional and marketing content in one message converts the entire SMS to marketing in regulators’ eyes.
The clinical evidence is strong. A meta-analysis of 16 randomized controlled trials (N=2,742) found that text messaging doubled the odds of medication adherence (OR 2.11, P<0.001) and increased adherence rates by 17.8 percentage points.
Tailored messages – those that reference the patient’s specific regimen rather than generic reminders – outperformed generic messages, and longer campaigns (6+ months) outperformed short bursts. For pharmacies, this reframes SMS from a marketing channel to a clinical intervention with measurable impact on refill behavior.
10-Digit Long Code (10DLC) is the US carrier registration system for Application-to-Person SMS. Since February 3, 2025, all A2P traffic in the US must be registered with The Campaign Registry. Unregistered messages are throttled or blocked by carriers.
Pharmacies don’t usually register directly, the SMS platform handles submission. What you should verify: the brand registration reflects your legal pharmacy entity, and the campaign use case is correctly classified (marketing vs. account notification). Misclassified registrations are a compliance problem even if nothing shows up in the inbox of the recipient.
GDPR requires two consent layers for pharmacy marketing SMS in the EU. First, a lawful basis for processing the phone number itself – for marketing, this almost always means explicit consent under Article 6(1)(a). Second, a separate ePrivacy consent for the SMS channel specifically. Opting into email does not authorize SMS.
Both consents must be freely given, specific, informed, and unambiguous, and withdrawal must be as easy as granting consent. GDPR Article 9 additionally classifies health data as a special category so medication names and treatment details stay out of SMS bodies in the EU just as they do under HIPAA in the US.








